Asthma Mortality
Deaths due to asthma are uncommon but are of serious concern because many of them are preventable. Although most deaths certified as caused by asthma occur in older adults, comparisons of mortality rates have tended to focus upon children and younger adults, among whom the diagnosis of asthma death is more accurate, because alternative diagnoses such as chronic obstructive pulmonary disease (COPD) are less common. Over the past 50 years, mortality rates in these younger age groups have fluctuated markedly in several high-income countries (HICs). Changes in medical care for asthma, especially the introduction of new asthma medications, potentially contributed to these epidemics of asthma deaths.
International comparisons
Asthma is a rare cause of mortality, contributing less than 1% of all deaths in most countries. Asthma death rates increase markedly from mid-childhood to old age and the majority of asthma deaths occur after middle age. Since there is considerable potential for diagnostic confusion with other forms of chronic respiratory disease in the older age groups, comparisons of mortality rates tend to focus on children and younger adults.
In 2016, the Global Burden of Disease collaboration estimated that 420,000 people in the world died from asthma – more than 1000 per day. International mortality statistics for asthma are limited to those countries reporting detailed causes of death. Figure 1 compares the age-standardised mortality rates for asthma among countries reporting asthma separately in two recent 5-year periods (2001-2005 and 2011-2015). This figure excludes some of the less populous countries, with fewer than 100 asthma deaths in either period. However, among the more populous countries there is an almost 100-fold variation in age-adjusted rates, between Italy (low) and Fiji (high).
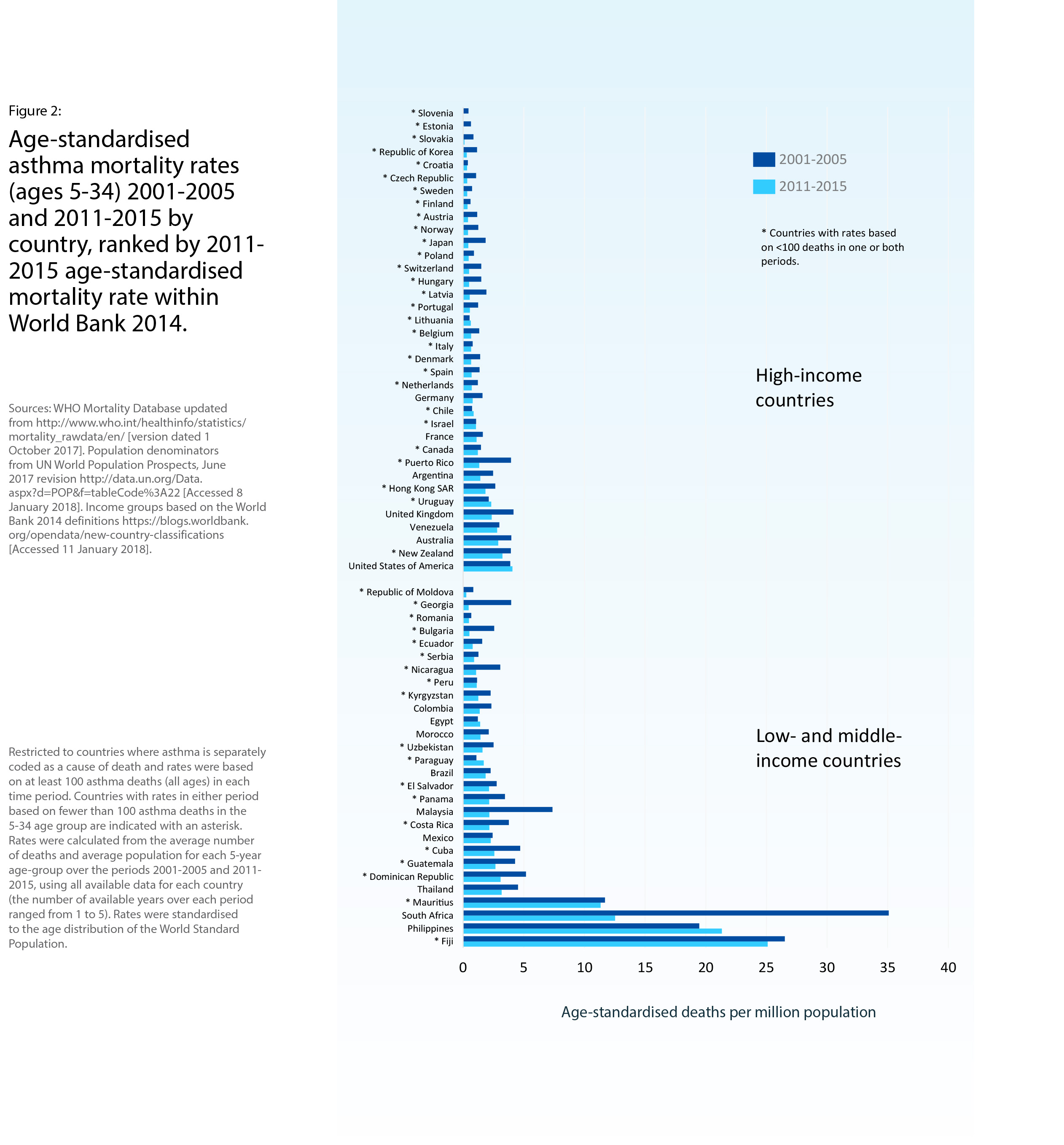
When the comparisons are limited to 5-34 year olds (Figure 2), deaths are fewer and margins of error are greater, but the large disparities persist.
Trends over time
Figure 1 shows that age-standardised death rates from asthma have fallen substantially (by about one-half ) in most countries from 2001-2005 to 2011-2015. This decline is generally reflected in the age group 5-34 years, including most of the 16 countries with more than 100 asthma deaths in this age group in both 5-year periods (Figure 2).
Over the past half-century, there have been two distinct peaks in early asthma mortality in many higher-income countries. The first occurred during the mid-to-late 1960s, with an approximately 50% increase in asthma death rates among 5-34 year olds. Researchers attributed this peak in asthma mortality to the introduction of high-dose isoprenaline inhalers as an asthma reliever medication, which can have toxic effects on the heart during acute asthma attacks. When these inhalers were withdrawn, the 1960s epidemic of asthma deaths subsided.
The second epidemic, during the mid-1980s, represented an increase of approximately 38% in asthma death rates among 5-34 year olds. In at least some of the affected countries, it was probably due to the widespread use of fenoterol, another inhaled asthma medication with potential cardiac toxicity.
Relationship of mortality to other measures of the burden of asthma
Taking a 50-year perspective, the epidemics of asthma mortality bear little relationship to the time trends for asthma prevalence or hospital admission rates for asthma. In several HICs asthma admission rates among children rose to a peak in the 1990s, after the 1980s peak in asthma mortality. Both hospital admission rates and asthma mortality rates among children have been declining since 2000, whereas asthma prevalence has been stable or rising in many countries (Chapter 4, Figure 3).
Figure 3 compares recent changes in agestandardised rates of mortality and hospital admission for asthma in 24 European countries reporting both measures during 2001-2005 and 2011-2015. Death rates declined more (in relative terms) than did admission rates, but there was very little correlation between these national trends.
When national asthma mortality rates for children were compared with asthma symptom prevalence and severity data for ISAAC Phase One centres in the same countries, a significantly positive correlation was found between childhood asthma mortality and the prevalence of more severe asthma symptoms in both 6-7 year olds (29 countries) and 13-14 year olds (38 countries). Such comparisons need to be interpreted with caution, because ISAAC centres are not necessarily representative of the countries in which they are located.
Avoidable factors in asthma deaths
Although asthma mortality rates have declined in many higher income countries, confidential enquiries in the United Kingdom have suggested that avoidable factors still play a part in most asthma deaths.
The most recent comprehensive review, of 195 asthma deaths in the UK during 2012-2013, found that nearly half died without seeking medical assistance or before emergency medical care could be provided, and the majority were not under specialist medical supervision during the year prior to death. Only one quarter had been provided with a personal asthma action plan, acknowledged to improve asthma care, and there was evidence of excessive prescribing of short-acting reliever medication, under-prescribing of preventer medication, and inappropriate prescribing of long-acting β2-agonist (LABA) bronchodilator inhalers as the sole form of treatment.
These observations, from a HIC with a tradition of evidence-based medicine and a national health service which is free at the point of use, suggest that improved access to appropriate asthma medication is a key goal in reducing asthma mortality worldwide.
Conclusion
Asthma deaths represent the “tip of the iceberg” with respect to the global burden of asthma. Although the risk of any individual person with asthma dying of their disease is thankfully very low, continued surveillance of asthma mortality rates is essential to monitor progress in asthma care and as an early warning of epidemics of fatal asthma, as have occurred in the past half-century.