Hospital Admissions for Asthma
Hospital admissions for asthma are often used as a target indicator of improvements in asthma care, but we have poor understanding of the factors underlying variations in hospital admission rates. Admission to hospital during an asthma attack may indicate the first asthma episode or a failure of preventive care for established asthma. Hospital care may be important to prevent a fatal outcome in severe or troublesome asthma. Historically, the relationship between asthma prevalence, severity and admission rates in high-income countries (HICs) has been complex, but changes in the admission rate over time correlate, albeit imperfectly, with changes in the prevalence and severity of childhood asthma.
International comparisons
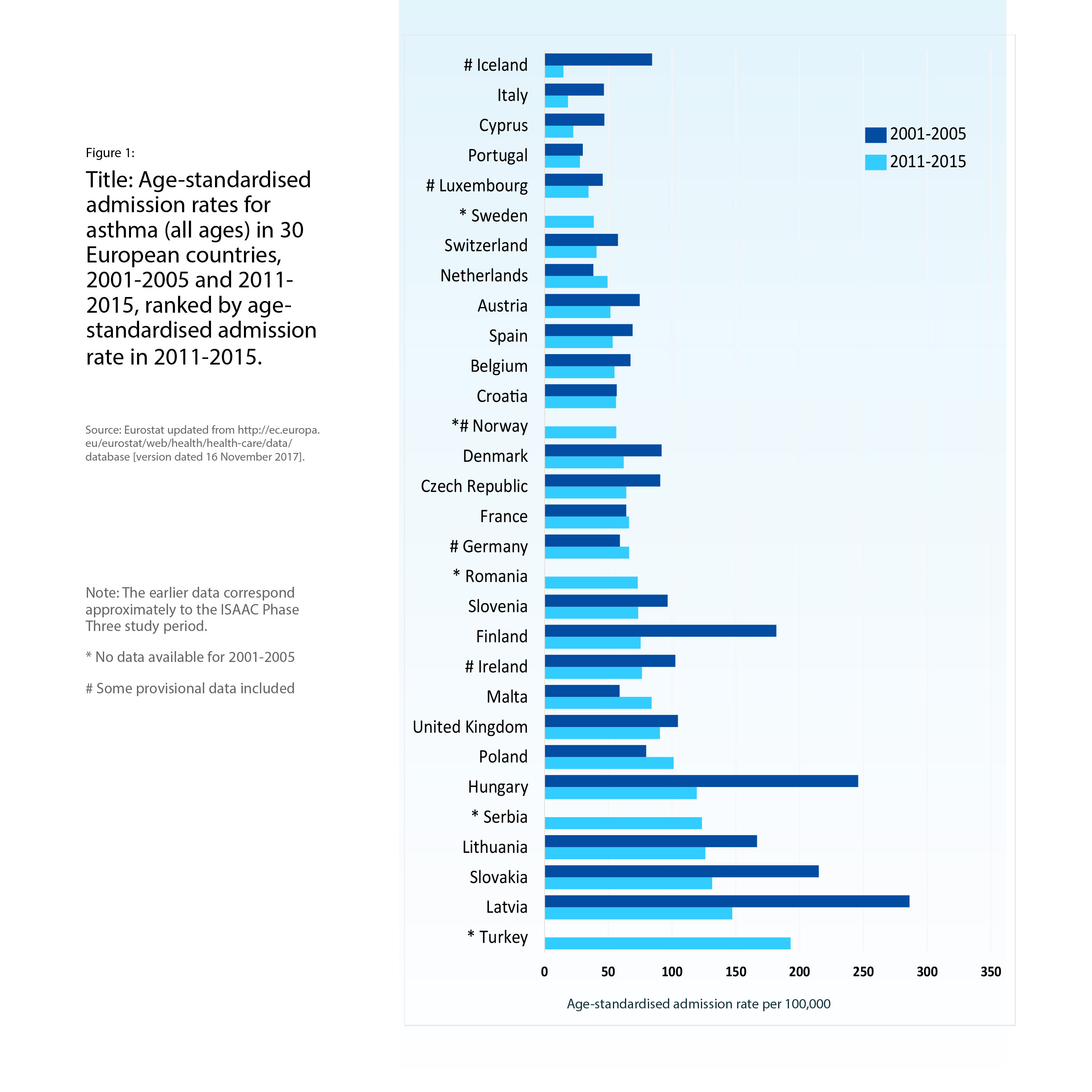
Many attacks of asthma are mild and selflimiting. The proportion of acute episodes resulting in hospital admission varies greatly, both within and between countries. Factors affecting hospital admission rates include the accessibility and affordability of the healthcare system, and the local thresholds for referral from community to hospital and from outpatient clinic or emergency room to inpatient care. National hospital admission statistics are lacking for most low- and middle-income countries. Hospital admissions and discharges for asthma are usually similar, as death in hospital is rare. In Europe, asthma contributes 0.6% of all hospital admissions and 0.4% of inpatient bed-days. However, rates vary by up to 10-fold between countries (Figure 1) and there is considerable variation between hospital admission rates for children (where rates are generally higher) and adults. It is important to exercise caution when interpreting geographical differences and trends over time in asthma admission rates for pre-school children (where diagnostic overlap with other wheezing illnesses may occur) and for older adults (where chronic obstructive pulmonary disease (COPD) may be confused with asthma).
Trends over time
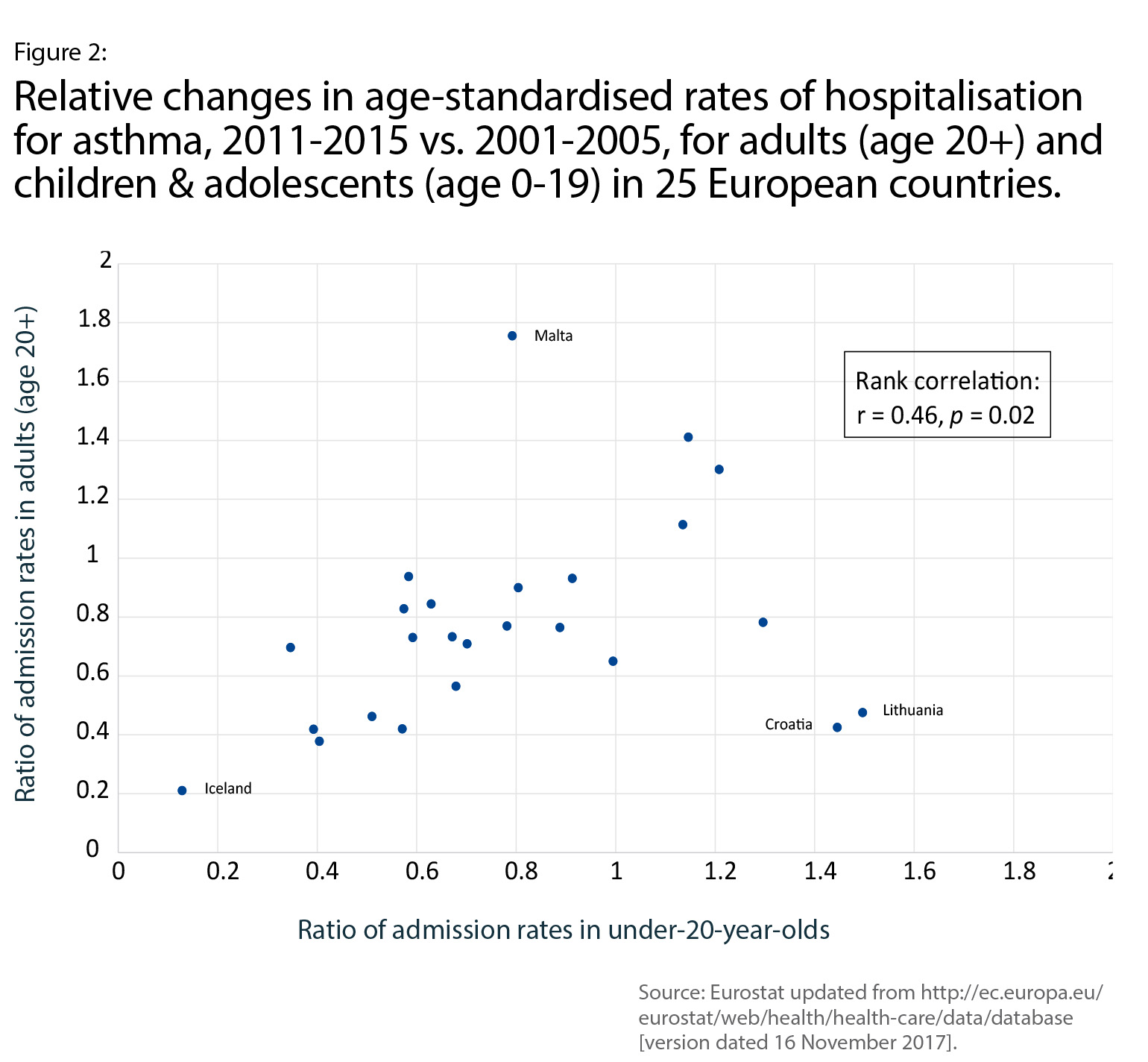
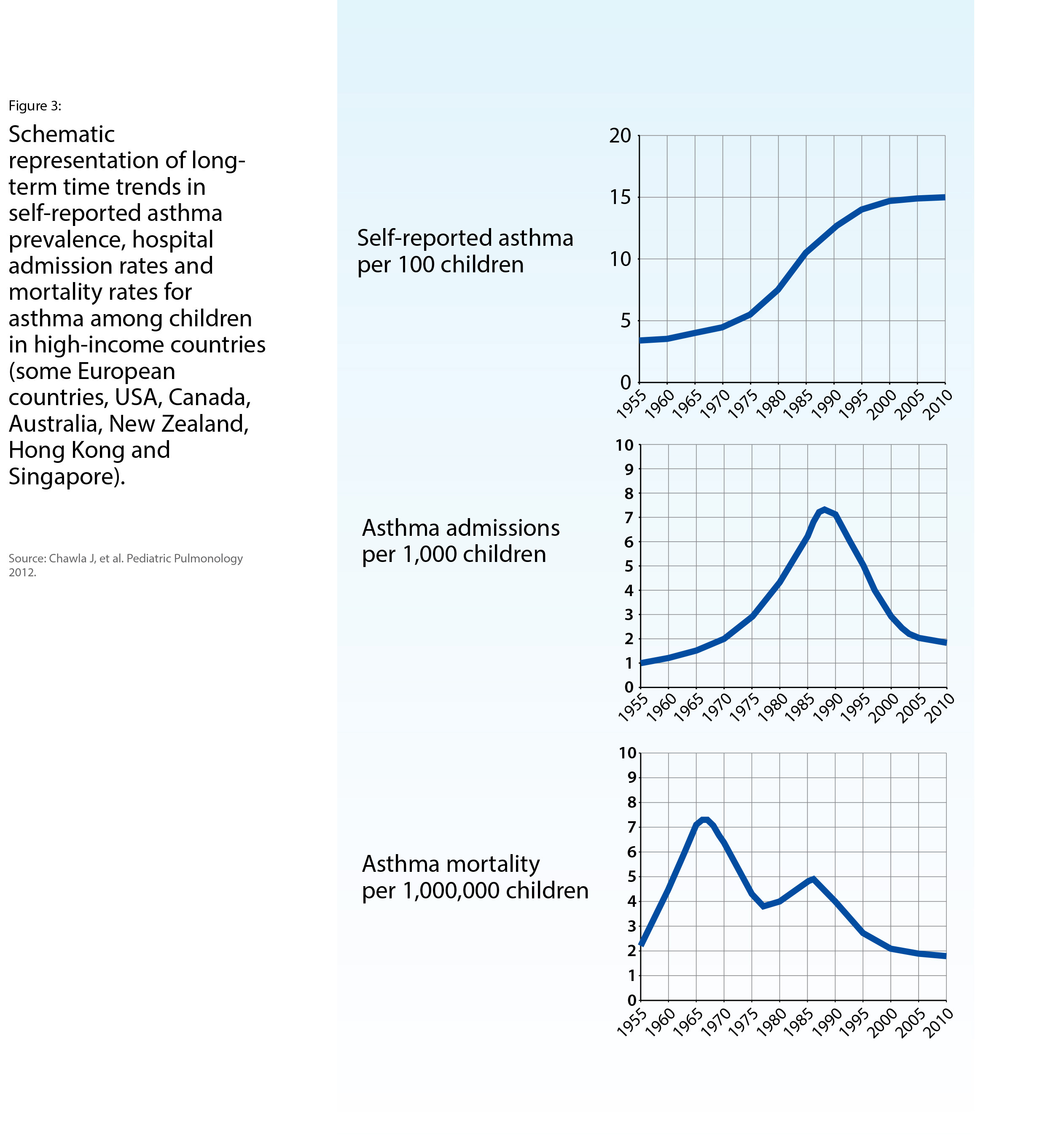
In most European countries (Figure 1), agestandardised asthma admission rates from 2001-2005 to 2011-2015 declined, with an over two-fold reduction in some countries. Adult and child/adolescent admission rates declined to a similar degree (Figure 2). The continuing decline in asthma admission rates among children is part of a longer-term rise and fall, which peaked in several HICs the early 1990s (Figure 3). Taking a 50-year perspective, the ‘epidemic’ of asthma admissions bears no temporal relationship to two epidemics of asthma mortality (in the 1960s and the 1980s, discussed in Chapter 5), nor to time trends of self-reported asthma prevalence (Figure 3). However, data from the United Kingdom showed a peak of primary care contacts for acute asthma, particularly among children, in the early 1990s, similar to that of asthma hospital admissions. This suggested a rise and fall in the incidence of asthma attacks in the community, rather than simply a change in patterns of referral to secondary care, or a reduction in the severity threshold for admission to the hospital ward.
An international comparison of time trends in asthma admissions and asthma drug sales in 11 countries during the 1990s found that increased inhaled corticosteroids (ICS) sales were associated with a decline in hospital admission rates for asthma. During the 1980s, ICS became more widely used for asthma prevention, however hospital admission rates for children increased during this period. Thus, it is not possible to draw firm conclusions about the extent to which uptake of effective ‘preventer’ medication has reduced hospital admission rates for asthma in HICs.
Relationship of hospital admissions to other measures of the burden of asthma
Data from centres participating in the International Study of Asthma and Allergies in Childhood (ISAAC) Phase One (1993-5) found that national asthma admission rates correlated with the prevalence of more severe asthma symptoms in 13-14 year olds, but not in 6-7 year olds. In contrast, there were no significant correlations between national admission rates and measures of asthma prevalence and severity in children participating in ISAAC Phase Three (2001-3). Cautious interpretation is required, however, because ISAAC centres are self-selected and are not necessarily representative of the countries in which they are located. Additionally, betweencountry comparisons at a single point in time
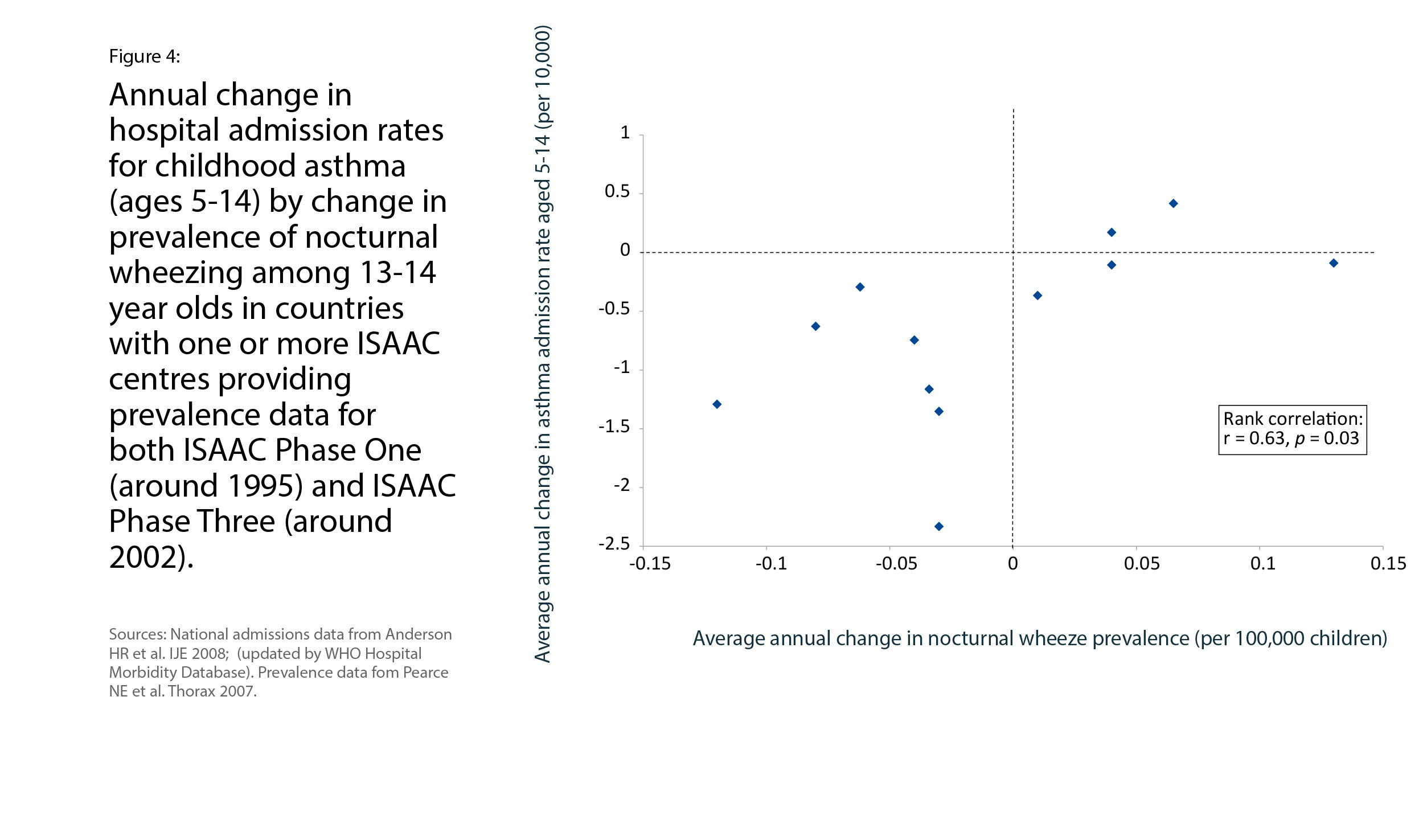
have significant potential for bias. However, some of these biases become less relevant if withincountry changes are examined over time. For countries with ISAAC study centres participating in both Phase One and Phase Three, national admission rates for childhood asthma declined in all except Hong Kong and Poland. This admission rate decline correlated with a decline in the prevalence of severe asthma symptoms over a similar period (Figure 4). In contrast, comparison of within-country changes in asthma mortality and admission rates for 24 European countries over the decade 2001-2005 through 2011- 2015 (Chapter 5, Figure 3) shows no correlation between time trends. Over this period, national age-standardised death rates for asthma reduced more, in relative terms, than age-standardised admission rates.
Conclusion
Asthma admission rates have been proposed as a target indicator for monitoring progress towards improved asthma care. Large reductions in admissions have occurred already over the last decade in several countries.
Currently, routinely collected asthma admissions information is almost entirely restricted to HICs, limiting the value of admission rates for surveillance of the global burden of asthma.
In countries that routinely collect admissions data, change in hospital admissions over time may be used as an indirect indicator of the burden of more severe asthma. More countries need to collect admissions data before admission rates can be used as an indirect indicator of the global burden of severe asthma.