Global Burden of Disease due to Asthma
How many people have asthma?
Establishing the proportion of the population who have asthma (that is, the prevalence of asthma), and comparing this prevalence between countries, requires the use of standardised measures implemented in large-scale, global surveys. Fortunately, we have this information from separate surveys of asthma in adults and children, but the last surveys were about 15 years ago. Questionnaires were used to measure asthma prevalence in these surveys. Although this method has some limitations as an accurate way of identifying the presence of asthma in individuals, it provides reasonable estimates of prevalence in populations and has the advantage of being feasible for large-scale surveys.
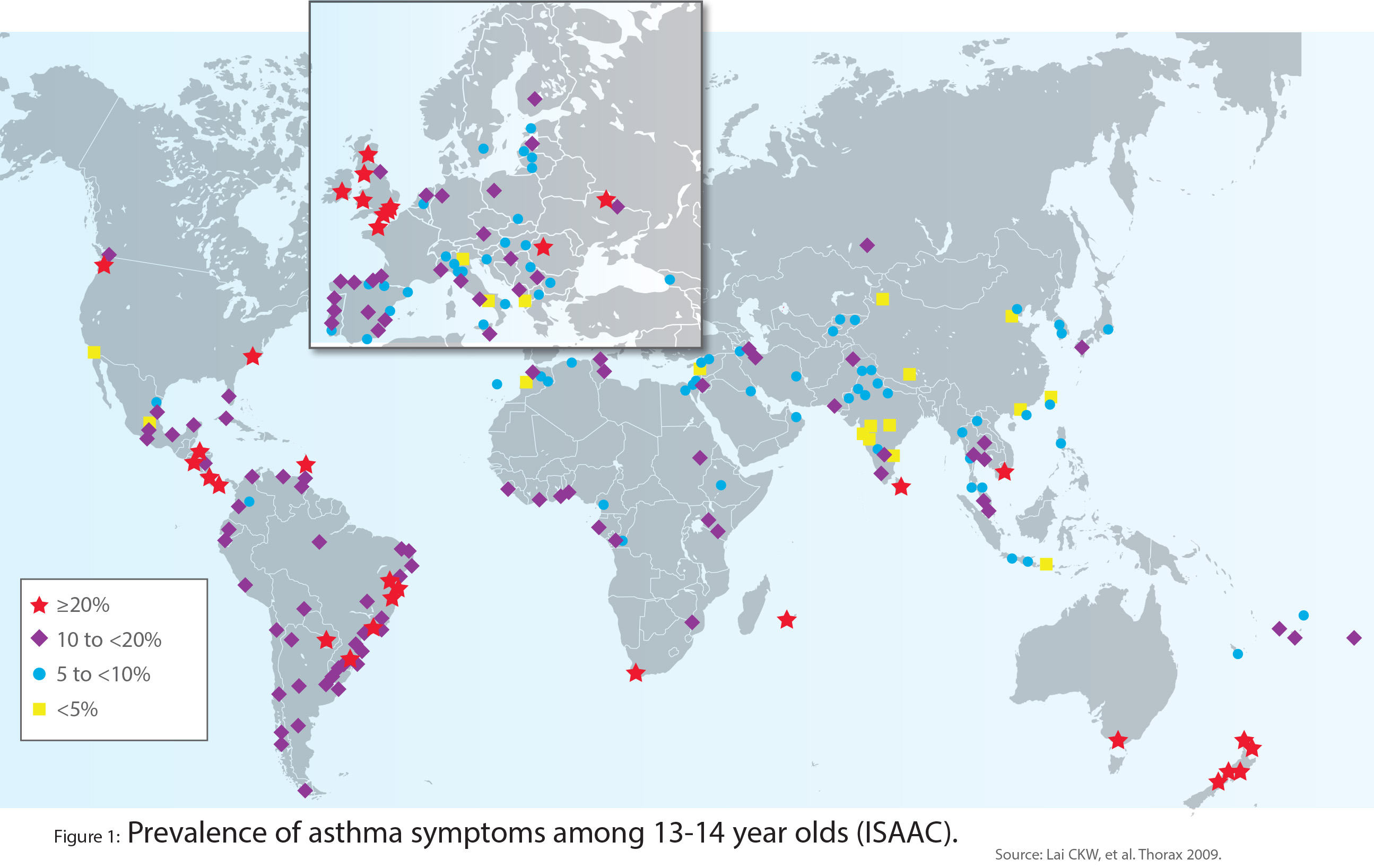
The International Study of Asthma and Allergies in Childhood (ISAAC) surveyed a representative sample of 798,685 adolescents aged 13-14 years in 233 centres in 97 countries between 2000 and 2003. In ISAAC these adolescents were asked whether they had experienced wheeze, a symptom that is commonly attributable to asthma, in the preceding 12 months. The crucial finding was that the prevalence of recent wheeze varied widely between countries and between centres within countries (Figure 1). The highest prevalence (≥20%) was generally observed in Englishspeaking countries of Australasia, Europe and North America, and in parts of Latin America. The lowest prevalence (<5%) was observed in the Indian subcontinent, Asia-Pacific, Eastern Mediterranean, and Northern and Eastern Europe.
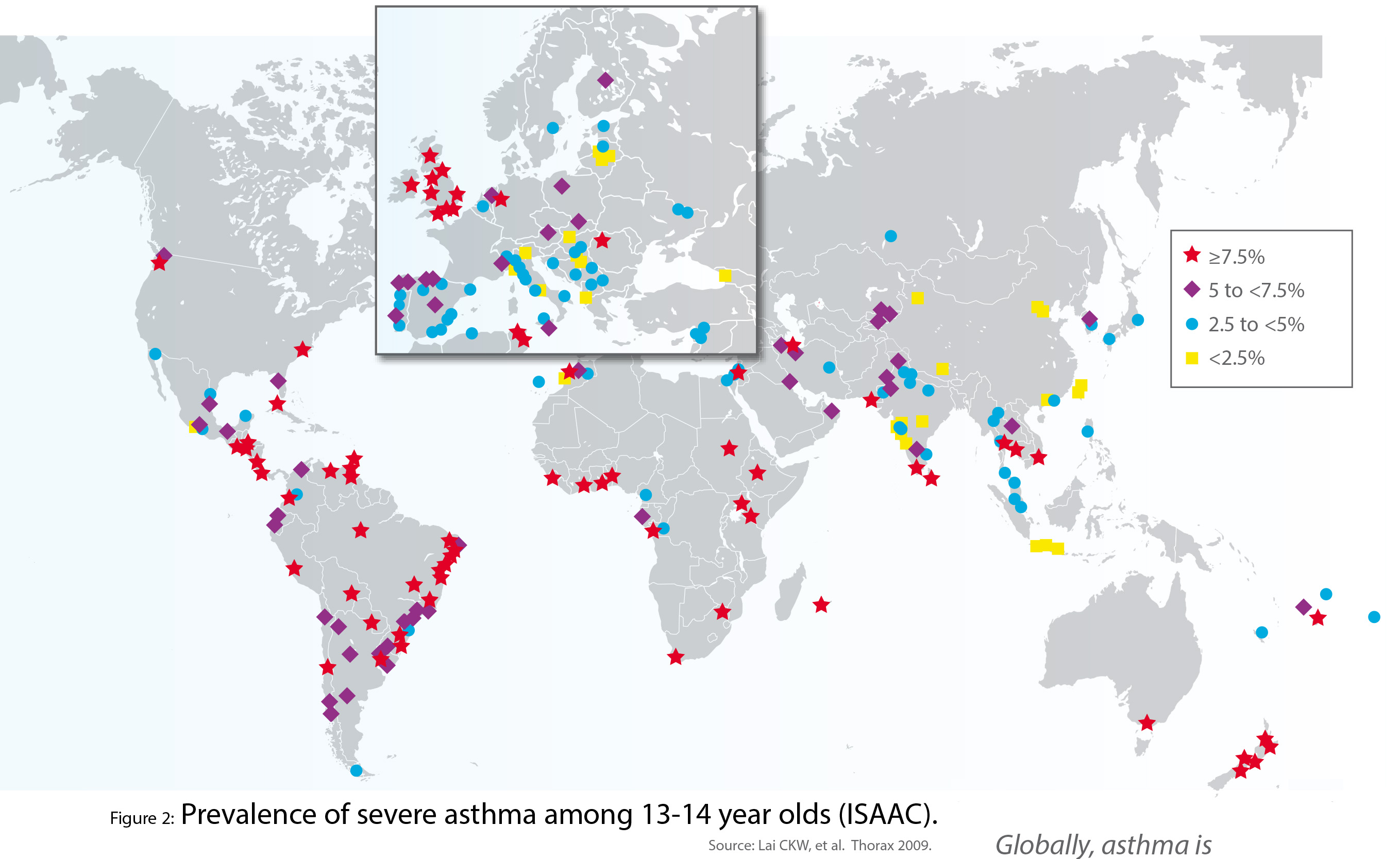
In this same survey, the prevalence of symptoms of severe asthma in the preceding 12 months (four or more attacks of wheeze, waking at night with asthma symptoms one or more times per week, and/or any episodes of wheeze severe enough to limit the ability to speak) also varied substantially, but was ≥7.5% in many centres (Figure 2).
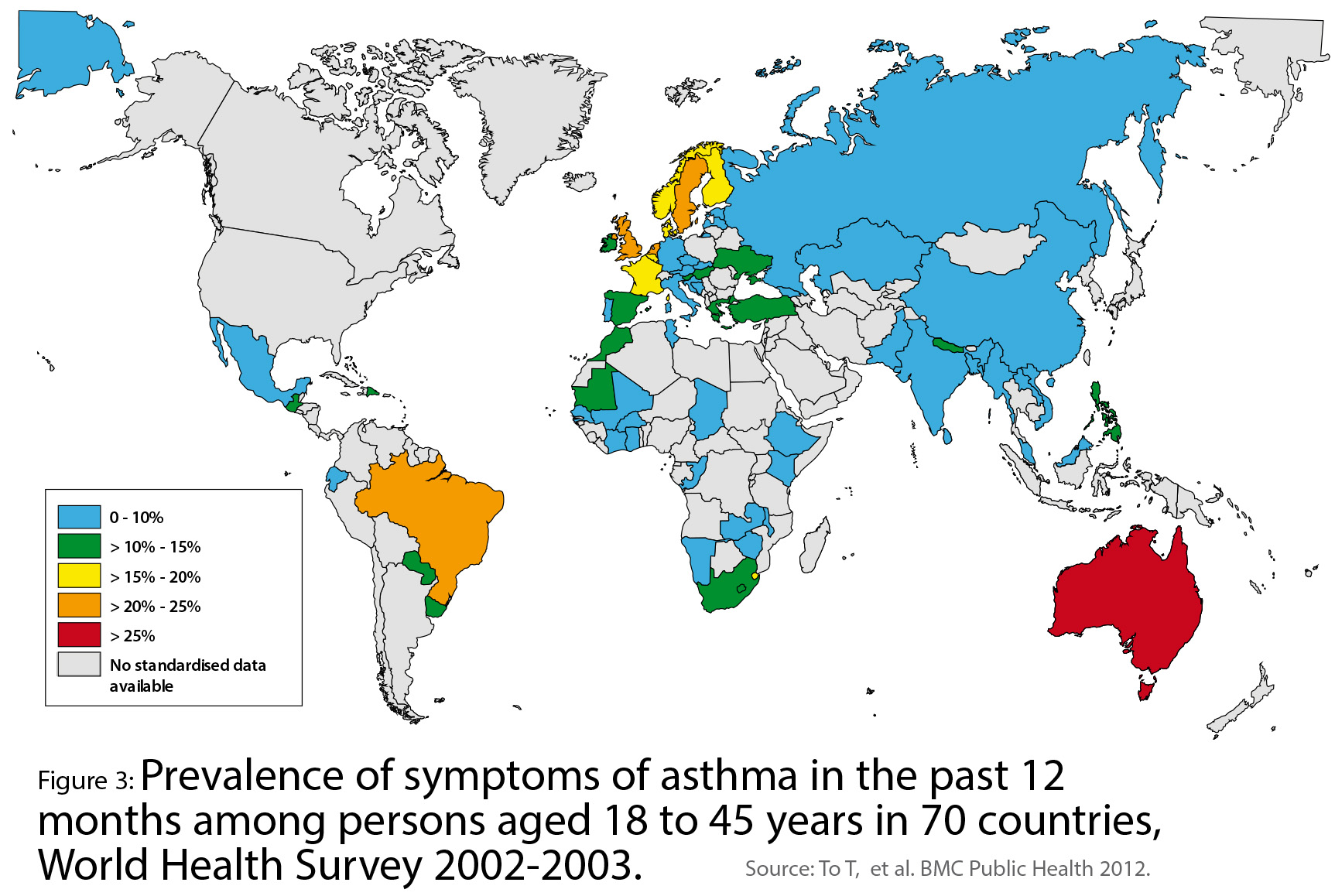
The prevalence of asthma in younger adults, aged 18-45 years, was estimated using data from the World Health Survey conducted by the World Health Organization (WHO) about the same time as ISAAC (2002-2003), in 177,496 adults living in 70 countries. As observed in children, the overall prevalence of asthma varied widely in younger adults. Overall, 4.3% of the global population in this age group reported a doctor’s diagnosis of asthma, 4.5% reported either a doctor’s diagnosis or that they were taking treatment for asthma, and 8.6% reported that they had experienced attacks of wheezing or whistling breath (symptoms of asthma) in the preceding 12 months (Figure 3). Australia, Northern and Western Europe, and Brazil had the highest prevalence.
The Global Asthma Network (GAN) is continuing the work of ISAAC. GAN Phase I (Chapter 1), based on the ISAAC methodology, will provide new data on asthma prevalence and severity in children (6-7 years), adolescents (13-14 years) and adults (parents or caregivers) around the world, and GAN expects to report their findings by 2020.
Researchers know much less about the prevalence of asthma in middle-aged and older adults including the elderly. This reflects both a paucity of survey data and the greater difficulty of distinguishing asthma from other respiratory conditions, such as chronic obstructive pulmonary disease (COPD), in older age groups. In 2016, the Global Burden of Disease (GBD) study estimated that there were 339.4 million people worldwide affected by asthma. This represents a 3.6% increase in age-standardised prevalence since 2006.
What is the impact of asthma on disability and premature death?
Burden of disease is a measure of health loss attributable to specific diseases. The GBD study has used mortality statistics and health survey data, where available, to estimate, for many countries of the world, two components of disease burden: Years of Life Lost due to premature death (YLL) and Years of Life lived with Disability (YLD). The latter quantifies both the extent of disability and its duration. Disability Adjusted Life Years (DALYs) are the sum of YLL and YLD. The GBD study publishes new analyses every few years and the 2016 findings are the basis of the estimates cited below.
In 2016, asthma, across all ages, contributed 23.7 million DALYs globally. This total burden of disease has remained unchanged since 1990, despite the substantial increase in world population over that time. Hence, the agestandardised rate (329·2 DALYs per 100,000 population in 2016) has decreased by 36% since 1990. Globally, asthma ranked 28th among the leading causes of burden of disease and 27th in low- and middle-income countries (LMICs).
More than half (56%) of the global burden attributable to asthma was due to 13.2 million YLD. This represents a small (3.0%) increase in the age-standardised rate of YLD due to asthma since 2006. In 2016, asthma ranked 16th in the leading causes of YLD globally.
Worldwide, there were 10.5 million YLL attributed to asthma-related premature deaths. This represents an age-standardised rate of 148·5 YLL per 100,000 population, 26% lower in 2016 compared to 2006. In 2016, asthma ranked 23rd (global) and 31st (LMICs) among the leading causes of premature mortality (YLL).
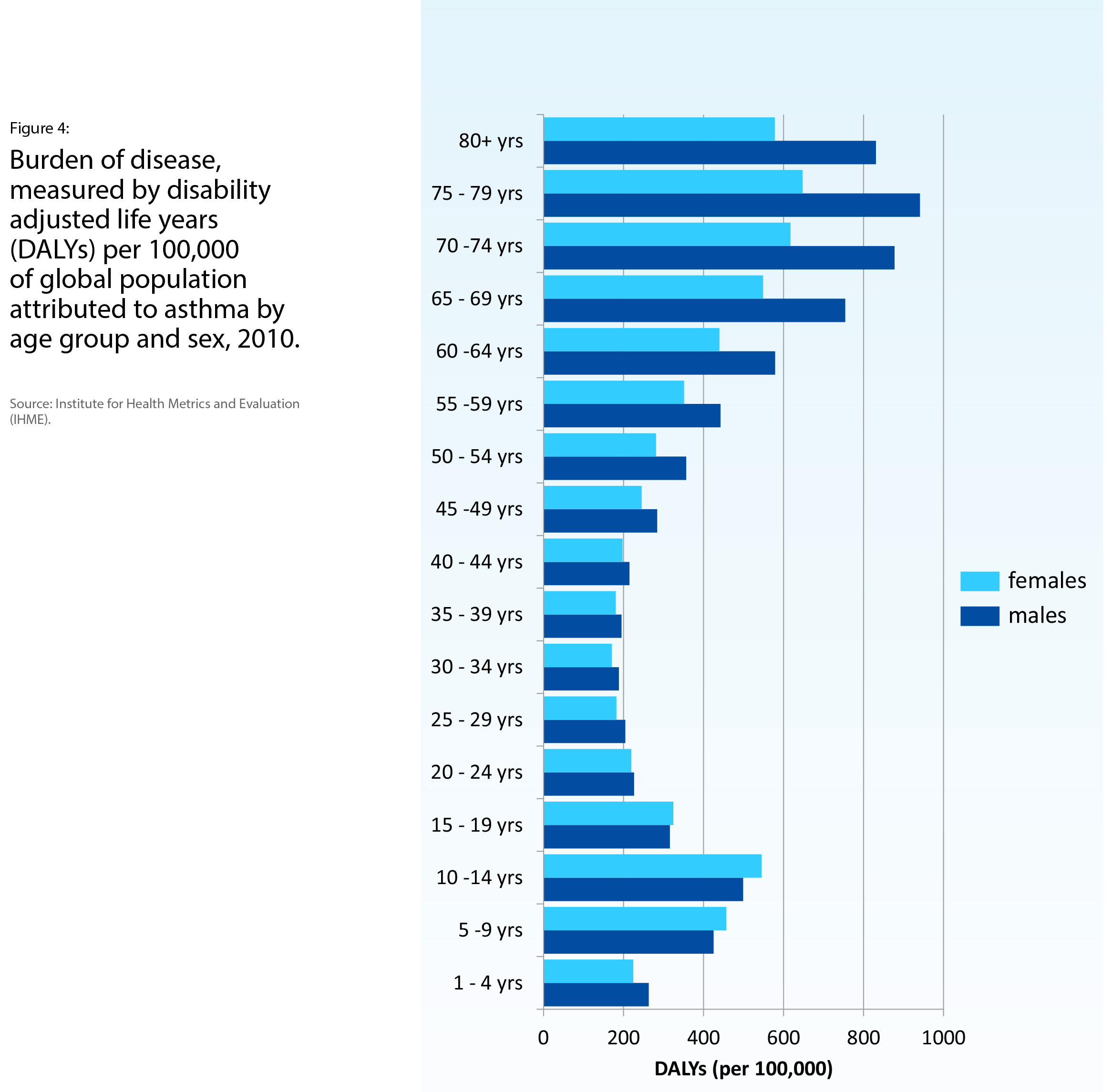
The age distribution of the burden of asthma, represented as DALYs per 100,000 persons, follows a bimodal distribution with peaks at age 10-14 years and at age 75-79 years (Figure 4). The lowest burden occurs at age 30-34 years. The burden is similar in males and females at ages below 30-34 years. However, in older adults, the burden is higher in males and increases with age (Figure 4).
What further information do we need about the burden of asthma?
Tracking the global burden of asthma depends on the acquisition of new standardised data over time for relevant parameters including, at least, prevalence, disability and mortality. It is becoming clear that asthma is a heterogeneous disease, with diverse causes, life-courses, outcomes and optimal treatments (Chapter 2). In further work on the burden of asthma, including both disability and premature mortality, it would be useful to link this burden to avoidable causes and treatable traits. This would highlight the potential value of interventions to prevent asthma and mitigate the consequences of asthma with effective treatment.