Achieving Access to Affordable, Quality-Assured, Essential Asthma Medicines
Asthma, once diagnosed, can be managed well with inhaled medicines of proven efficacy: preventer inhaled corticosteroids (ICS) for more frequent symptoms and reliever bronchodilator for acute symptoms. Patients with asthma need uninterrupted, affordable and quality-assured supplies of these medicines, yet many do not have these; challenges and solutions are put forward here.
World Health Organization Essential Medicines
Until 2017, the World Health Organization (WHO) Model List of Essential Medicines (EML) included two ICS and one short-acting β2-agonist (SABA) for asthma. In 2017 a combination ICS and rapidly-acting long-acting β2-agonist (LABA) was added, the latter giving symptom relief and thus encouraging adherence to ICS. Recent evidence suggests that, in people with mild asthma, combination budesonide–formoterol, used as needed for symptoms, may be as effective as ICS, used regularly twice daily, together with SABA used as needed for symptoms. However, at present, combination inhaler devices are more expensive than ICS and SABA devices, which may limit the use of this regimen. Indeed many countries, especially low- and middle-income countries (LMICs) do not yet have ICS and bronchodilators on their national EML, and many are not providing them free or subsidised for patients. Thus there is an urgent need to address essential asthma medicine-related measures at both country and global levels.
Several studies show that there is limited access to affordable, quality-assured essential asthma medicines in many LMICs. The WHO Non-Communicable Disease (NCD) Global Action Plan 2013-2020 set an 80% target for availability of essential NCD medicines in both public and private facilities by 2025. We have not reached this target for asthma medicines, with little progress to date.
The WHO EML 2017 includes three medicine groups for asthma:
- (i) ICS aerosol: beclometasone dipropionate (50μg and 100μg), and budesonide (100μg and 200μg)
- (ii) one combination ICS and LABA: dry powder budesonide with formoterol two dose strengths: 100μg with 6μg, 200μg with 6μg
- (iii) one bronchodilator: salbutamol sulphate in these formulations: metered dose inhaler: 100μg, respirator solution for use in nebulisers: 5mg/mL, and injection: 50μg/mL in 5mL ampoule.
Quality assurance
Asthma inhalers are among the most complex medical devices manufactured by the pharmaceutical industry in widespread use. They require accurate manufacturing so that they deliver the required dose in particles of the right size to reach the lower airways. The WHO EML states “It is the responsibility of the relevant national or regional drug regulatory authority to ensure that each product is of appropriate pharmaceutical quality”. This is vital for asthma inhalers.
To be safe and efficacious, asthma inhalers need to comply with international quality standards. Although many inhalers may meet these standards, some in the marketplace do not. The WHO Prequalification Programme is a centralised quality assessment initiative that has achieved greater access for millions of patients to quality-assured medicines for other selected diseases. Unfortunately asthma inhalers are not included in this programme, but it is time they were.
Access is limited
Many LMICs do not have essential asthma medicines on their EML or National Reimbursement List (NRL), and some do not have them on either list. The 2013-14 Global Asthma Network survey of 111 countries found that, among LMICs, only about half had ICS on their EML and NRL. People with asthma in the LMICs with no NRL and those with an NRL but no ICS on it are likely to have very poor access to affordable, quality-assured ICS. A 2012 survey within 52 LMICs found ICS availability was particularly poor in national procurement centres and main hospitals, and some countries were applying very high margins on these medicines.
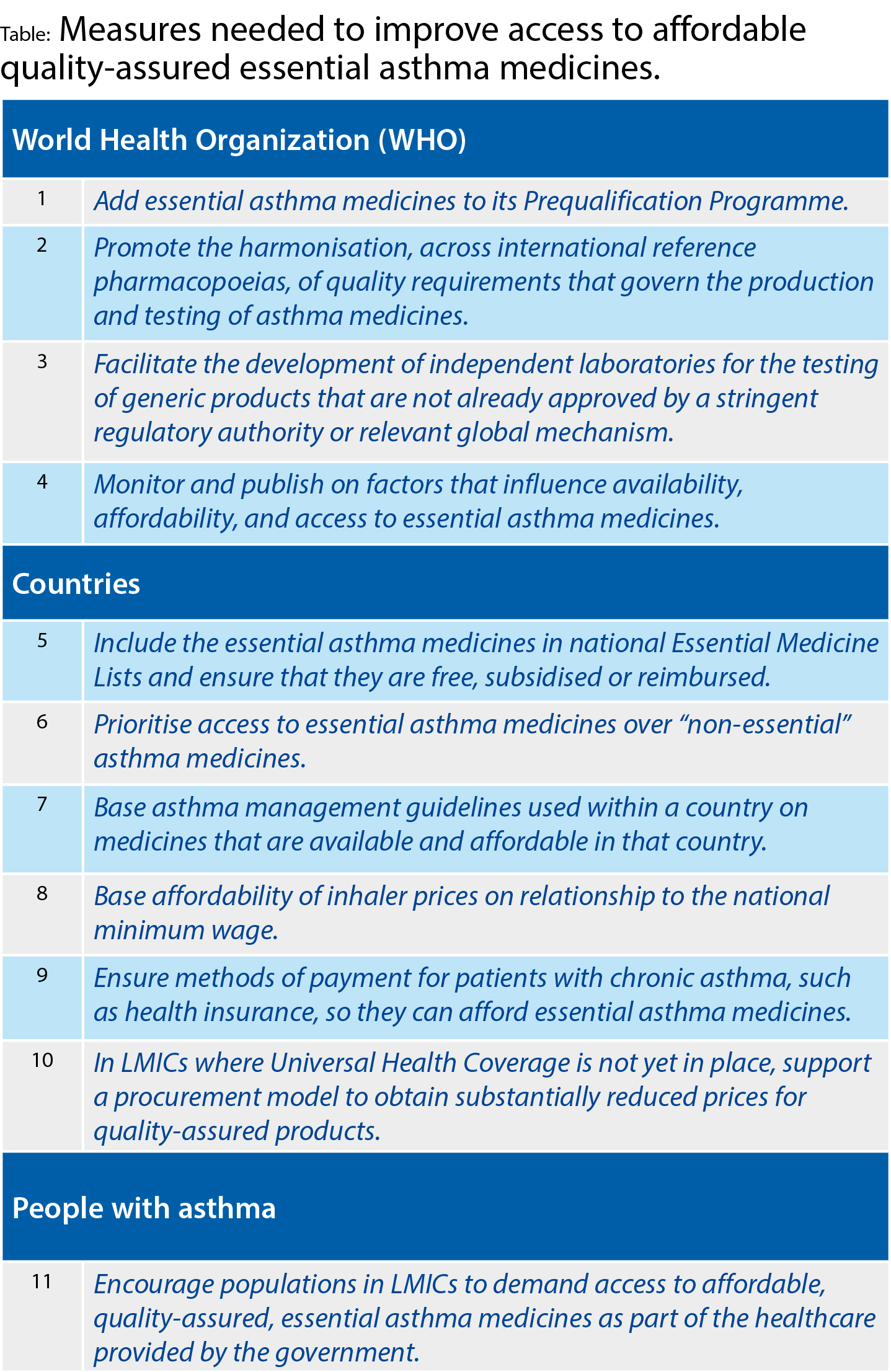
Solutions The International Union Against Tuberculosis and Lung Disease (The Union) developed the Asthma Drug Facility (ADF) as a practical solution to these issues and this was operational from 2006 to 2013. The ADF provided quality-assured medicines with independent testing of inhalers; lower pricing through a competitive process; financing strategies using the Global Fund to Fight AIDS, TB and Malaria, Revolving Drug Funds (after an initial capital investment, medicine supplies are replenished with monies collected from the sales of medicines) and health budgets; asthma guidelines and training materials; and the monitoring of asthma outcomes, such as emergency visits and hospitalisations. It is vital that the supply within countries of affordable, quality-assured, essential asthma medicines is guaranteed and uninterrupted to achieve effective asthma management for everyone needing it. Countries may need to work on how their national policies, programmes, example, address asthma medicines, as well as how medicines are procured and made available to patients. In most countries, the funding of essential asthma medicines competes with the funding for very expensive asthma medicines that benefit asthma patients not responding to essential asthma medicines. For the greater good, however, prioritisation of essential asthma medicines is vital. Countries need to base national asthma management guidelines on medicines that are available and affordable in their country. It is vital that countries ensure access to medicines at all levels of healthcare, especially among poor and marginalised populations. In low-income countries, authorities should develop methods of payment for people with chronic asthma, such as health insurance and ZAKAT (Islamic Relief Worldwide), so they can pay for their medicines. The Table summarises measures aimed at improving access to affordable, quality-assured, essential asthma medicines.Conclusion
Now that the WHO EML includes the ICS/LABA combination-inhaler, there is further potential to improve asthma management. Nevertheless, many countries have not yet included the essential medicines recommended by the WHO on their own EMLs and many do not subsidise these asthma medicines, especially in LMICs. ICS, the main asthma preventers, which lead to improved asthma control and reduction in the burden of asthma, are less commonly supported by governments than the short term reliever inhalers, and this needs to be corrected.